
African Research Journal of Education and Social Sciences, 5(2), 2018
Elias Mseti
Assistant Lecturer
Faculty of Arts and Social Science, the Open University of Tanzania,
Kawawa raod-Kinondoni, P. O. Box 23409, Dar-es-salaam-Tanzania
Corresponding Author Email: msetielias@gmail.com
Jazila Mgweno,
Kibaha Designed Public Hospital
Registered Nurse
Email: jazilamgweno@yahoo.com
Abstract: The occupational chemical exposures have been observed to cause high morbidity and mortality in the World. This study examined exposure to hospital disinfectant chemicals and health effects among nurses in selected Kibaha town health facilities in Tanzania. The study focused on establishing the association between commonly used hospital disinfectant chemicals and reported health effects among nurses. The study used cross sectional survey design. Purposive sampling procedure was used to arrive at the sample of two hundred and two health attendants from two health facilities. Data were collected using structured questionnaire. Data were entered, cleaned and formatted using Microsoft excel and then transferred to Statistical Packages for Social Sciences (SPSS Version 20) for analysis. Findings obtained from questionnaire revealed the level of association between working in stations which frequently used disinfectant chemical and health effects of chemical exposure. The study provides a platform for other researchers to conduct further investigation on the exposure to hospital disinfectant chemicals and health effects among nurses.
Keywords: Hospital Disinfectant Chemicals, Hospital chemical exposure, Chemical health effects, Nurses chemical exposure
1.0 INTRODUCTION
Occupational chemical exposures have been observed to cause a high morbidity and mortality in the World (WHO, 2003). This is caused by the increase of chemical content in commercial and manufactured products. The chemicals are inhaled and ingested by people who are near the chemical industries or those using chemicals (Prüss-Ustün, Vickers, Haefliger & Bertollini, 2011). The inhalation and ingestion of these chemicals have negative health effects. Centers for Disease Control and Prevention, 2007-2008 reported that chemicals are pervasive in all aspects of patients’ lives, whether found in the air, water, soil, foods or consumer products.
Exposure to these chemicals has adverse effects to the human body. National Cancer Institute (2008-2009) reported that chemical babies born by smoking women are exposed to chemicals’ adverse effects. Women transfer the chemicals to children by exposing themselves to chemical substances used in households or at work. Prenatal exposure to certain chemical is linked to increased health consequences that can manifest across the lifetime of an individual and can potentially be transmitted to next generation (Wingle, Turner & Knewisk, 2009). Shinwell (2001) stated that there is an increase of health effects caused by pesticides and other hazardous chemical in the developing countries, this has been influenced by development of private enterprises such as small and medium size work place, increase of industries located in residential areas and the movement of industrial harmful dust or wastes.
Aboud, Chuwa, Abassy, Makbel, Karugendo, Abdallah et al., 2005 reported that most dangerous activities are carried out by health attendants like nurses and medical attendants. These activities such as dressing, surgical procedures and cleaning are reported to cause skin diseases and burns. This is because during those actions toxic chemical agents such as disinfectants, antiseptics, homicidal, anesthetic gas and sterilants are used (Manyele, Ngonyani & Eliakimu 2008).
In developing countries like Tanzania, health workers are highly exposed to chemicals as most of the working environments have no sufficient protective equipment (Shinwell, 2001). Prüss-Ustün et al. (2011) further stated that health care workers are highly exposed to chemicals either knowingly or unknowingly, this increases the risk of getting health effects resulted from chemical exposures. According to Tanzania health demographic survey report (OSH, 2005), health care workers’ are trained on occupational health safety but the health facilities are not adhering to health, safety and security standards putting health workers at risk of chemical exposure. Therefore, there is a need for regular and continuous data collection to determine the change in type and magnitude of health risks caused by disinfectant chemical exposure in hospitals and setting appropriate actions on its prevention.
Health professionals are prone to hospital disinfectant chemical exposure; they are always in contact with these chemicals and other related materials in the work places. The manufacture and use of industrial chemicals increased in 1970’s, it is reported that more than 15 folds are imported and exported worldwide (Wilburn & Eijkemans, 2004). In Tanzania the management and control of Occupational safety and health at workplace provided several measures to overcome the problem of chemical exposure. The measures include; provision of knowledge and skills on health and safety to health workers, inspection of premises, assisting on certification during compensation and emergency reporting when there is incident (OSH, 2005). Manyele et al. (2008) stated that the status of occupational safety among health service providers in the Hospitals of Tanzania is still low, the hospitals use chemicals like Alcohol 70-90%, aqueous iodine 3%, Chlorhexadine gluconate and cetrimide.
Health facilities in Kibaha Town like other health facilities in Tanzania have the environment which may provide risk of hazardous activities due to chemicals. Workers’ safety and health procedures in health facilities have not identified exposure to disinfectant chemicals as a concern. There is little or no documented data on the safety and health of nurses, this is a challenge in ascertaining whether the safety and health risks are present or not (Manyele & Anicetus, 2006). Against this background, this study intended to examine the issue of exposure to hospital disinfectant chemicals and health effects among nurses in Kibaha Town Health Facilities, Tanzania.
2.0 METHODOLOGY
This study adopted cross-sectional survey research design. A cross sectional survey design was found appropriate for getting information at one point in time to describe the current characteristics of the selected samples from each of the participants (Creswell, 2014). The study was conducted in Tumbi hospital and Mkoani health center which are both government health facilities. Tumbi Hospital and Mkoani health center were selected due to their accessibility. The study population comprised of the health care providers from two government health facilities, Mkoani health center and Tumbi hospital, in Kibaha Town.
The study population included Nurses and Medical attendants aged 25-60 years, clinicians, pharmacist technicians and facility unity supervisors. There was no gender preference. Tumbi hospital and Mkoani health center has a total of 231 and 46 staff members respectively. A total of 170 participants were drawn from 231 health care providers of Tumbi hospital and 32 participants from 46 health care providers of Mkoani health center. An average of 100 participants were taken from 122 health care providers (nurses and medical attendants) who engage in the activities which use disinfectant chemicals (direct handling chemicals) and 98 participant were drawn from 155 health care providers (clinicians, part of nurses and pharmacy technicians) who indirectly handle the disinfectant chemicals. Questionnaire and observation were the main data collection instruments used. In the questionnaire both open and close ended questions were prepared and administered to medical attendants who are exposed to Hospital chemicals. The questionnaire aimed at assessing the area of exposure (Skin, Nose and mouth) and variables expected to affect the musculoskeletal and respiratory systems.
After data collection from the field, the researcher coded data from text to numerals and keyed them into MS excel by double entrants and later cleaned them to remove errors and to facilitate accuracy and consistence. Each possible answer was assigned a number to ease the determination of accuracy of data during the whole process of data entry and cleaning. Then, analysis of the clean data was done using Statistical Package for Social Science (SPSS) according to research objectives.
3.0 RESULTS
3.1 Prevalence of musculoskeletal and respiratory health effects
Results obtained from questionnaire reported that few respondents (24.8%) suffered from musculoskeletal problems, skin problems, skin allergy, skin burn and skin irritation while slightly more than a three quarter of respondents (75.2%) had no musculoskeletal problems or skin problems. Furthermore, 11.3% had experienced respiratory health effects such as asthma, nose and throat irritations while majority of the respondents (88.7%) never experienced respiratory problems.
The study found a weak correlation between the use of personal protective equipment and the incidents of chemical exposure. A significant association (p<0.05) was found on exposure to hospital disinfectant chemicals and health effects experiences among nurses. The study found that those who had direct and indirect chemical contact experienced health effects the p-value on musculoskeletal was 0.039, respiratory 0.013.
3.2 Association between exposure variables and health effects
Hospital disinfectant chemicals have multiple health effects. In this study musculoskeletal health effects and respiratory problems will will be considered. Table 1 shows the association between exposure variables and musculoskeletal effects.
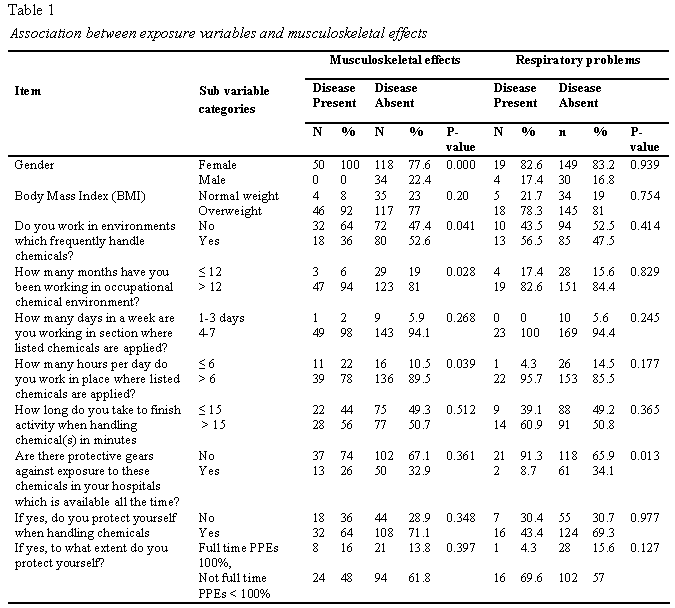
Results obtained from questionnaire indicated that musculoskeletal problems were significantly associated with working in the stations which involved handling disinfectant chemicals compared to stations which do not handle disinfectant chemicals frequently (p=0.041), exposure to disinfectant chemicals for more than 6 hours per day caused musculoskeletal problems as compared to individuals with less than 6 hours of exposure per day (p=0.039) and exposure to disinfectant chemicals for more than 12 months caused musculoskeletal problems as compared to less than 12 months exposure (p=0.028). Also, respiratory problems were significantly associated with the lack of use of personal protective equipment (p=0.013).
4.0 DISCUSSION
Results obtained from questionnaire based on self reported health problems including musculoskeletal and respiratory health effects associated with occupational exposure to disinfectant chemicals among nurses and other health attendants working in two selected health facilities in Kibaha town. Exposure routes reported by nurses and other Health Care Workers (HCWs) included chemical contact through skin, eyes, nose and mouth. According to the Body Mass Index (BMI) results, many health care workers working in selected Health Care Facilities seemed to be overweight which is dangerous because according to Stern & Lagos, (2008) overweight people are more exposed to health effects than peoples with normal weight.
Foremost, the relation between exposure variables and selected health outcomes was examined using chi-square test and the results with p-value ≤ 0.05 indicated strong associations between variables and p-value > 0.05 indicated weak or no association between variables (Figueiredo, Woodley, Brown & Ross, 2013). This study results noted that; more than 70% of medical attendants who reported to have experienced selected health effects in their life, were Nurses from the stations which frequently use disinfectant chemicals. Besides, many respondents from work stations reported to have inadequate supply of personal protective equipment. They also reported that they eat and drink at the same workplace where chemicals are used. Manyele et al. (2008) reported that eating and drinking in chemical induced places is dangerous. The reported health problems by respondents were associated with direct contacts with chemicals such as Jik, Lysol and other sterilants and detergents. The study also found severe chemical exposure effects among individuals who used more than three chemicals on their daily working activities. The highest exposure time was from seven to twelve hours per day and the reported activities performed frequently included decontamination, sterilization and cleanliness.
Nevertheless, available information from the previous study conducted by Bamidele, Adeoye, Ntaji & Oladele, 2014 in South Nigeria demonstrated that; systematic exposure to disinfectant chemicals increases the risk of health effects such as musculoskeletal and respiratory problems alike the results of this study which also revealed significant association between disinfectant chemicals and respiratory. Although prevalence of such diseases is very low, the result of this study revealed musculoskeletal problems were significantly associated with working in the stations which handled disinfectant chemical frequently as compared to those stations which do not handle disinfectant chemicals frequently. Moreover, it was reported that chemicals used in hospitals particularly antiseptics and disinfectants might cause skin problems. However, this study revealed low prevalence rate of self reported musculoskeletal health effects; skin burn was 10.4%, irritation 15.4% compared to the study conducted in Nigeria by Bamidele et al. (2014), which reported 17.5% and 22.6% of skin burn and skin irritation respectively.
In comparison with other studies, grouping direct and indirect users of disinfectant chemicals in this study was a problem due to the fact that, it is very difficult to identify cadres which are indirectly exposed to chemicals because many cadres among HCWs are directly exposed to the use of disinfectant chemicals due to frequent inter-changing of activities in different work station and too many unforeseen events like accidents which sometimes necessitate some workers to move from the stations which are not highly exposed to the use of disinfectant chemical to stations which are highly exposed (Stern & Lagos, 2008). Also due to the low availability of personal protective equipment (PPE) and poor safety practices the level exposure to disinfectant chemicals and its related health effects are more frequent.
5.0 CONCLUSIONS
In comparison with other studies, critical findings of this study revealed that, there is significant association between disinfectant chemicals and musculoskeletal and respiratory health effects;p<0.039 and p<0.013 respectively. A few respondents reported that, skin irritation, skin burn and dermatitis were among musculoskeletal health problems affecting them, while irregular period, heavy menses and amenorrhea were the mentioned reproductive health effects and chest problems. Asthma and nose and throat irritation were mentioned as respiratory health effects. Similarly delayed conception, uterine fibroid, infertility, abortion, fetal defect, newborn defect, breast new growth, fibroid and infertility were the notable hormonal health effects.
Comprehensive action is required to be taken in all hospitals, in order to ensure that they protect themselves when handling hospital chemicals. Likewise, hospital workers should avoid eating and drinking while handling chemicals in hospitals. There should be media campaigns, education, and legislation to inform all hospital workers to be part of a comprehensive strategy to advice hospital workers and increase their understanding on adverse health effects of hospital chemical exposure among hospital workers.
REFERENCES
Aboud, S. M., Chuwa, A. A., Abassy, M., Makbel, A. M., Karugendo, E. N., Abdallah, O. I., … & Sanga, C. (2005). Tanzania Demographic and Health Survey 2004-2005.
Bamidele, J. O., Adeoye, O. A., Ntaji, M. I., & Oladele, E. A. (2014). Occupational hazards exposure and their resultant effects on hospital attendants in health facilities of a local government area in South-South, Nigeria.
Centers for Disease Control and Prevention (2009). National Health and Nutrition Examination Survey (NHNES) 2007-2008.
Creswell, W. J. (2014). Research design. Qualitative, quantitative, and mixed methods approaches. Los Angeles: Sage.
Figueredo, A. J., Woodley, M. A., Brown, S. D., & Ross, K. C. (2013). Multiple successful tests of the Strategic Differentiation-Integration Effort (SD-IE) hypothesis. Journal of Social, Evolutionary, and Cultural Psychology, 7(4), 361.
Manyele, S. V., Ngonyani, H. A. M., & Eliakimu, E. (2008). The status of occupational safety among health service providers in hospitals in Tanzania. Tanzania journal of health research, 10(3), 159-165.
Manyele, S. V., & Anicetus, H. (2006). Management of medical waste in Tanzania hospitals. Tanzania Journal of Health Research, 8(3).
National Cancer Institute. (2009). Cancer Trends Progress Report. Retrieved from https://progressreport.cancer.gov/sites/default/files/archive/reportMarch2015.pdf
OSH, (2005).Occupational safety and health: Tanzania Health Demographic Survey Report. Tanzania.
Prüss-Ustün, A., Vickers, C., Haefliger, P., & Bertollini, R. (2011). Knowns and unknowns on burden of disease due to chemicals: a systematic review. Environmental Health, 10(1), 9.
Shinwell, J. (2001). Occupational Health: Manual for Primary Health Care (WHO-EM/OCH/085/E/l/04/01/00) Cairo: Misri.
Stern, B. R., & Lagos, G. (2008). Are there health risks from the migration of chemical substances from plastic pipes into drinking water? A review. Human and Ecological Risk Assessment, 14(4), 753-779.
Wingle. DT, Turner. MC and Knewisk. D, (2009). A Systemic Review and Meta Analysis of Childhood Leukemia and Parental Occupational Pesticide Exposure. Environmental Health Perspectives 117.1505-13.
Wilburn, S. Q., & Eijkemans, G. (2004). Preventing needlestick injuries among healthcare workers: a WHO-ICN collaboration. International journal of occupational and environmental health, 10(4), 451-456.
World Health Organization (2003). Diet, nutrition and the prevention of chronic diseases. WHO
—